Some patients can now receive full text reports via the NHS App if their GP practice has enabled it.
Numerous of the specialty groups have recently received feedback from reporters that their report text has been pasted into ChatGPT for a ‘translation’, with the patient then directly contacting the identified reporter, usually out-of-hours, for inappropriate clinical discussion.
This is occurring as it seems follow-up appointments with specialists for correct and proper clinical discussion are now quite delayed and do not take place before the report appears on the App.
Some Radiology Reporters may not be expecting this kind of contact and some Trusts may not have a procedure on how to manage this process.
Structured reporting would go some way to mitigating this issue. Adding a ‘patient friendly’ summary in the report body likewise, but there seems to be no ideal solution at present.
I know provider discharge letters are meant to be written to the patient, to be understandable by the patient. I don’t know if this applies to radiology reports though? Certainly the ones I had recently weren’t, and I pasted them into Chat GPT to try and get a better understanding.
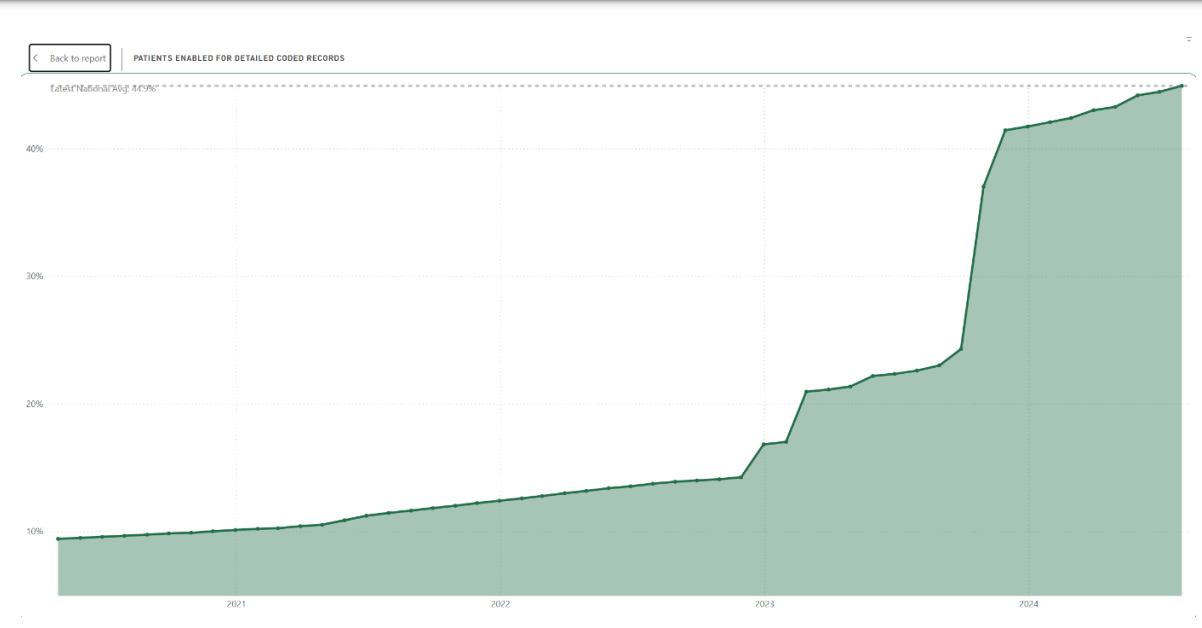
This slide produced by Redmoor Health, a consultancy working in the Primary Care digital transformation space, may help explain partly what’s going on [except that it’s for patient access to their GP detailed coded record, I can’t find the equivalent slide for patient access to letters filed by their GP].
I have always argued the correct workflow is the report only to be made visible to the patient once the report has been ‘endorsed’ i.e. read, acknowledged and acted on by the requesting or responsible clinician.
Dimitri, with the emergence of patient portals, the information is often available to the patient before the physician even has the chance to look at it. Not sure if that is not the case in the UK but if I assume it will follow what is happening here in the US. Just as an example, as a patient I have access to my labs, path reports and radiology reports typically in a day, my follow-up with the ordering physician is typically not within a couple of days at best. Now, I might need AI to “translate” the report into something I understand but that is a separate issue.
Hi Herman, very good point, yes, in the UK it has been generally somewhat unusual for the report to be available to the patient before follow-up in the past (and previously it wasn’t really made available for easy access at all). Across the NHS we’re having longer delays in scheduling appointments for follow-up or clinical consultations so that, combined with the ‘new’ NHS App functionality, has recently caused this to create these contacts with reporting staff.
A point which has just been raised to me and is quite important I guess - are PACS Managers aware there’s now a potential need to contact patients and clarify when a ‘wrong report’ is loaded and then removed or corrected in the department?
That’s not a step usually on our administrative housekeeping workflows…