Has anyone adopted a workflow for ingesting images into a PACS without the need for using the Radiology Ris. Do you have any advice or can you identify any potential issues.
Looking to solve
Non Radiology imaging were there is a lack of compliance for using the RIS.
Point of care imaging for open wounds in trauma.
Community wound care for evaluation/ documentation.
I think that depends on your PACS supplier. We use Sectra and it is possible to tag any interesting studies with whatever you want to create specific teaching folders which filter for those tags. I don’t know what the other PACS Systems provide.
In relation to point of care wound management, many PACS suppliers provide support for mobile devices, so you can store photos from your phone to the PACS. Again you would need to contact your PACS supplier.
On Carestream/Philips you can create studies directly on PACS without the need for a RIS entry. The issue here is that they perpetually show up as having no RIS sync in the PACS database (naturally). So if you are using worklists to identify errant studies that need to be matched back to a RIS order you have to continually disregard the intentionally non-RIS’d activity.
We just moved to Sectra, and know it’s possible but was not sure if you still needed an order to be sent in from somewhere or if images can just be ingested, linked to the correct patient and not flag as a mismatch or missing Ris entry.
Hi James. It would be useful to test that patient demographic updates propagate through to PACS?
The master patient administration system.PAS (hospital information/ADT) typically initiates the demographic updates. This takes into account manual updates entered on the PAS and also automated changes on name address etc fed into GP systems and shared through the spine demographic services PDS and strategic tracing service.
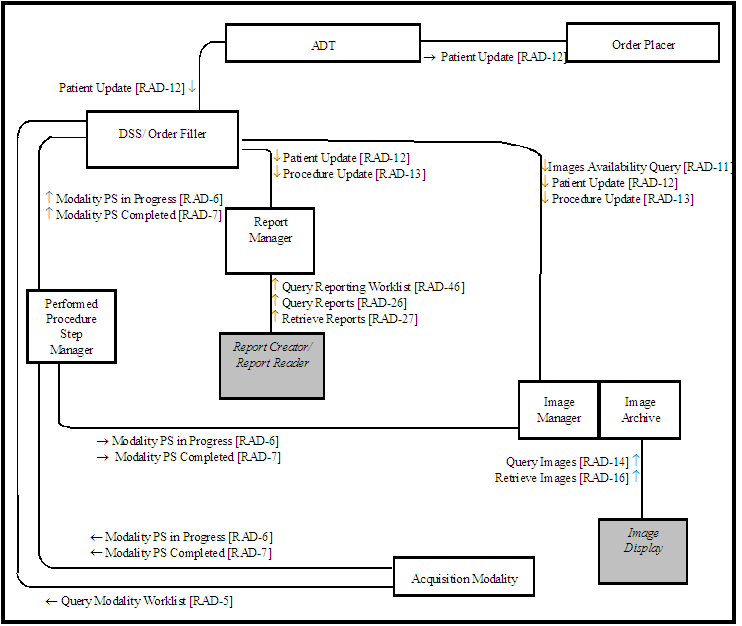
The standard IHE patient information reconciliation workflow is for these updates to be propogated from the PAS through the order filler / department system scheduler (aka RIS) to PACS.
This may still happen if the patient does not have a linked order entry - but it would be good to confirm.
We tried this for a while in a bid to prevent further duplication of GM radiology examinations. The problem was that the patient linking didn’t last long enough to keep the records merged creating confusion about whether the study had been imported or not. At the moment we have reverted back to previous practice of matching to a RIS entry.
Thanks @rhidian.bramley yes we need to ensure the EPR would update the demographics for patients without a RIS attendance. As long as it passes I guess they would remain in sync as both systems use the PAS as the Master id. May need to also to look at getting the id formats aligned with the RIS e.g site prefixes to prevent replication of the same id’s in the matching algorithm.
We had a brief discussion with Sectra about this a couple of years ago now where they could use our PAS system Medway to generate the DMWL to the modality and then send to PACS. We were thinking of using this workflow for Medical Photography but never started the project. As mentioned by other replies you would need to think about the exam coding and descriptions and BI.
We are hoping to implement a POCUS (US) workflow within the next 6 months or so. We have Sectra. Currently our orders are sent from EPR to RIS to PACS. This will change to EPR to PACS to RIS via new interface (which we will have to do anyway due to EPIC in a year or two). We are assured that Sectra can identify a POCUS order and will create the ‘packet’ in PACS without creating it in RIS. A DMWL will be sent to the modality and images sent to PACS. An auto-report will be generated and sent to EPR (not RIS). Lots of testing to be done to confirm though and fairly high costs.